Proprioceptive Neuromuscular Facilitation
- Proprioceptive neuromuscular facilitation (PNF) is an approach to the therapeutic exercise that uses proprioceptive, cutaneous, and auditory input to produce functional improvement in motor output and can be vital element in the rehabilitation process of many injuries.
- PNF techniques are used in sports medicine for increasing strength, flexibility, and coordination. The technique also decreases deficits in kinesthetic sense in response to demands placed on the neuromuscular system.
PNF Neurophysiological Principles
- Autogenic Inhibition: Inhibition mediated by afferent fibers of stretched muscle on alpha motor neurons resulting in muscle relaxation. In simple words, the stretched muscle relaxes with the golgi-tendon orgran (inhibitory impluses) overrides spindle (excitatory). This is taking advantage of the slow stretch principles that increases range of motion from a biophysical standpoint.
- Reciprocal Inhibition: Agonist received excitatory impulses but antagonist is inhibited.
- Successive Induction: Voluntary motion of one muscle can be facilitated by the voluntary motion of another.
Stretching Techniques
|
To produce muscle relaxation through an inhibitory response for increasing range of motion.
|
PNF Stretching Techniques
|
Contract-RelaxThe body part being stretched is passively moved until resistance is felt. The patient is told to contract the antagonist muscle isotonically. The movement is resisted for ten seconds or until the patient is fatigue. The patient relaxes for ten seconds and limb it passively moved to a new stretching position. This exercise is repeated three to four times. This is an example of Autogenic inhibition.
|
|
Hold-RelaxA technique similar to contract-relax; however, an isometric contraction of the antagonist is used. The patient moves the body part to resistance and holds position. Therapist isometrically resists muscle for ten seconds. Patient relaxes and limb is moved to new end range, either actively by the patient or passively by therapists. This exercise is repeated three to four times and an example of reciprocal inhibition.
|
|
Slow-Reversal-Hold-RelaxPatient moves body part in agonist pattern with isontonic contraction. Patient contracts with an isometric contraction of the antagonist. Patient relaxes the antagonists and then the agonists are contracted while stretched is being applied.
|
|
Strengthening Techniques
|
To assist patient in developing muscle strength, muscle endurance, and coordination.
|
PNF Strengthening Techniques
|
Rhythmic InitiationConsists of a progressive series - first passive movement, then active assisted movement, followed by active movement through an agonist pattern. This approach can be initiated within the first day following an injury. It helps patients with limited movement and progressively regain strength through the range of motion.
|
Repeated ContractionThis technique is used for muscle or muscle group weakness. The patient moves isotonically against the maximum resistance until he/she experiences fatigue. Once fatigue is felt, a stretch is applied to the muscle to facilitate greater strength production. The amount of resistance applied depends on the strength of the patient.
|
Slow ReversalPatient moves through complete range of motion against maximum resistance. The resistance is applied to both the antagonist and agonist muscle groups to ensure a smooth and rhythmic movement. The major benefit of this technique promotes normal reciprocal coordination of agonist and antagonist muscles.
|
Slow-Reversal-HoldThe patient moves a body part isometrically using the agonist muscle group. Immediately after the movement, an isometric contraction occurs. The patient is to hold at the end of each isotonic movement. The major benefit of this movement allows the patient to develop strength at a specific point in the range of motion.
|
|
Rhythmic Stabilization
This technique uses an isometric contraction of the agonists, followed by an isometric contraction of the antagonists. Repeated contraction of this motion promotes strengthening. |
|
Basic PNF Pattern Techniques
- The patient must be taught the PNF pattern movements from starting to ending position.
- When learning the patterns, the patient should watch moving limb for feedback on directional and positional control.
- Simple verbal commands should be initiated by therapists - push, pull, or hold.
- Hands contact can facilitate movement response.
- The therapist should use correct body mechanic when providing resistance.
- The amount of resistance applied should facilitate a maximum response from patient to allow smooth, coordinated movements.
- Rotational movements is vital during all PNF patterns
- The distal movements of the pattern should occur first and completed by the halfway point of movement.
- The stronger components are emphasized to facilitate the weaker components.
- Pressing the joint together increases stability; traction pulls the join apart and facilitates movement.
- Giving a quick stretch causes a reflex contraction of targeted muscle.
PNF Patterns
- The PNF exercise patterns involve three components: flexion-extension, abduction-adduction, and internal-external rotation.
- The patterns mimic a diagonal rotation of the upper extremity, lower extremity, upper trunk, and neck.
- The pattern activates muscle groups in the lengthened or stretched positions.
- The upper and lower extremities each have two patterns: D1 and D2 motions targeting flexion and extension.
- The patterns are used to improve range of motion at the joint as well as introduce resistance training. This will help improve the patients strength.
Upper Extremity Pattern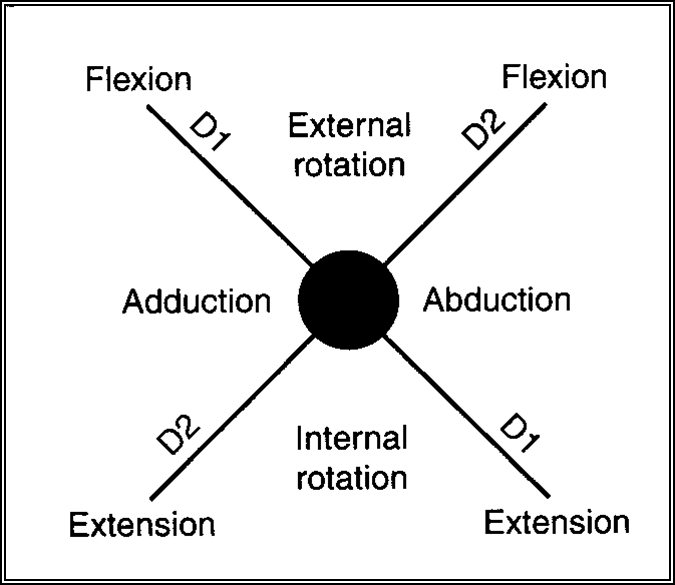
|
Lower Extremity Pattern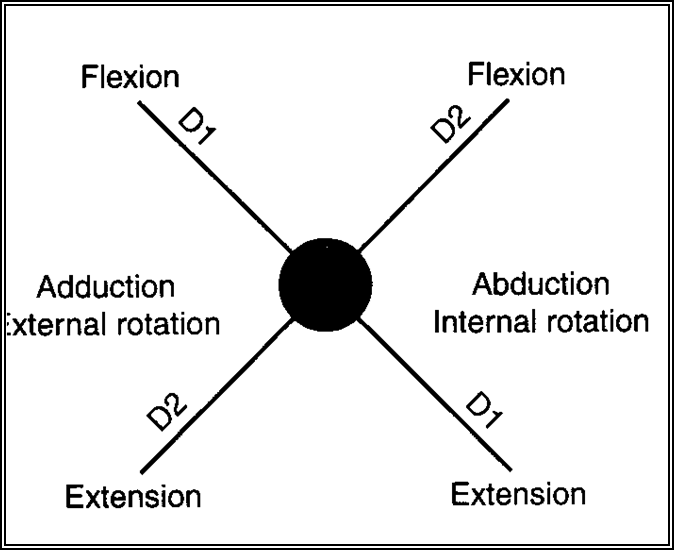
|
PNF Upper Extremity D1 Flexion/Extension PatternThe pattern mimics throwing a frisbee

D1 Flexion Pattern Starting Position
Upper Extremity D1 Flexion Starting Position
Hand Position
Movements to End Position

D1 Flexion Ending Position
D1 Extension Starting Position D1 Extension Starting Position
Hand Position
Movement to Ending Position

D1 Extension Ending Position
|
PNF Upper Extremity D2 Flexion/Extension PatternThe pattern mimics a reverse and regular throwing pattern.

D2 Flexion starting position
Upper Extremity D2 Flexion Starting Position
Hand Position
Movements to End Position

D2 Flexion Ending Position
D2 Extension Starting Position D2 Extension Starting Position
Hand Position
Moving to Ending Position

D2 Extension Ending Position
|
PNF Lower Extremity D1 Flexion/Extension PatternMovement is similar to the Figure 4 position

D1 Flexion Starting Position
Starting Position
Hand Position
Movements to Ending Position

D1 Flexion Ending Position
D1 Extension Starting Position Starting Position
Hand Position
Movements to Ending Position

D1 Extension Ending Position
|
PNF Lower Extremity D2 Flexion/Extension PatternMovement is similar to a wind-up kicking position

D2 Flexion Starting Position
Starting Position
Hand Position
Movements to Ending Position

D2 Flexion Ending Position
D2 Extension Starting Position Starting Position
Hand Position
Movements to Ending Position

D2 Extension Ending Position
|
